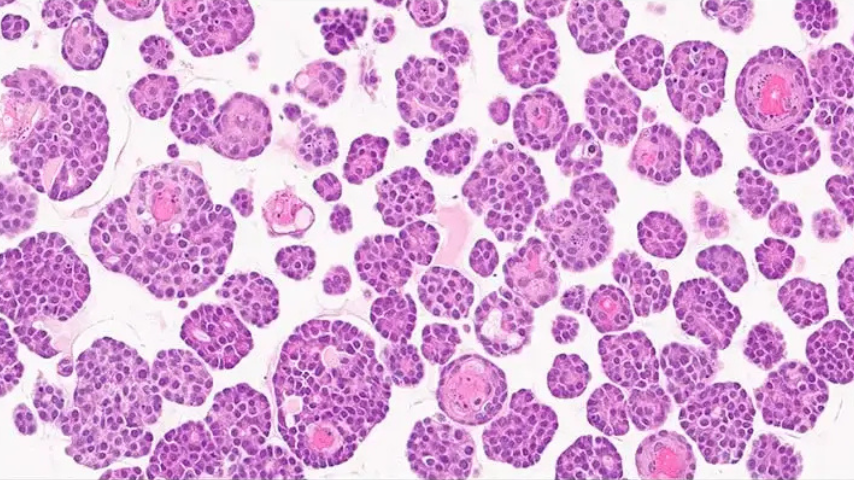
What are PDX-derived organoids (PDXOs)?
PDX-derived organoids, or PDXOs, are three-dimensional tumor models generated from clinically characterized patient-derived xenograft tumors. At Champions, these ex vivo models are designed to preserve meaningful tumor heterogeneity and support translational drug testing in biologically relevant advanced tumors.
How do Champions’ PDX-derived organoids differ from conventional patient-derived organoids (PDOs)?
Champions’ ex vivo platform is built from low-passage PDX-derived material and uses a matrix-free assay format with no added ECM. This allows us to study advanced, heavily pre-treated tumor biology in selected-model studies while avoiding added ECM that can complicate drug interaction and imaging readouts.
How quickly can an ex vivo study start?
TumorGraft3D supports practical study startup using banked, PDX-derived 3D tumor models rather than fresh patient tissue workflows. Standard selected-model studies can often move forward more efficiently than fresh-tissue approaches, while more customized study designs, such as target validation, advanced co-culture, or specialized endpoints, may require additional setup.
What tumor types are available in the ex vivo bank?
The TumorGraft3D bank currently includes CTG models across multiple cancer indications. Major categories include NSCLC, breast, colorectal, ovarian, sarcoma, and melanoma, with additional coverage in areas such as pancreatic, GBM, prostate, gastric, endometrial, HNSC, and RCC.
Can Champions’ PDX-derived organoids support screening studies?
Yes. TumorGraft3D supports selected-model screening and comparative ex vivo studies across biologically defined cohorts. Rather than broad exploratory HTS, the platform is best used for fit-for-purpose studies designed to compare assets, evaluate response patterns, and guide the next decision.
Are the models suitable for biomarker and mechanism-focused studies?
Yes. TumorGraft3D can support mechanism-focused and biomarker-informed studies when the assay fit is right. Depending on the question, studies can incorporate flow cytometry, NGS, qPCR, Western blot, and cytokine or soluble biomarker readouts to deepen biological interpretation.
Do the models support immune co-culture?
Yes. Co-culture studies can support fit-for-purpose questions around immune-mediated killing and microenvironment context. These studies can help probe whether immune context changes apparent activity versus monoculture, whether ADCC or other immune-mediated effects are detectable, and whether suppressive TME components shape response.
Why does a matrix-free format matter?
TumorGraft3D uses a matrix-free format with no added ECM. This matters because added ECM can introduce unpredictable interactions with complex modalities such as peptides and antibodies, and it can also create autofluorescence that complicates imaging-based interpretation.
How are Champions’ ex vivo models stored and prepared?
TumorGraft3D models are banked and prepared in a standardized ex vivo workflow designed for selected-model studies. Depending on the study design, models are thawed, seeded, and brought into the appropriate assay format before dosing and endpoint analysis.
How do PDX-derived organoids compare with PDX models?
PDX-derived organoids and PDX models are best viewed as complementary. Ex vivo studies can provide earlier comparative signal and help prioritize cohorts, assets, or hypotheses before in vivo work, while PDX studies remain important for questions that require full in vivo context, such as systemic biology, PK/PD, biodistribution, or certain linker-driven ADC questions.
Can these ex vivo models support radiopharmaceutical or radiation-based studies?
In the right study design, TumorGraft3D can support certain longer-window ex vivo questions where duration and tumor context matter. Fit should be assessed based on the modality, exposure window, and endpoint strategy so the study design matches the biological question.
Are studies customizable for specific research questions?
Yes. Champions works with clients to design studies around the scientific question, indication, biomarker profile, model set, and endpoint strategy needed to support a meaningful translational decision.
How are model quality and study fit assessed?
Champions’ ex vivo models are supported by baseline characterization and study-fit review before execution. Depending on the model and study type, this can include confirmation of human tumor content, molecular characterization, tissue-block availability, and readiness for the intended assay format so the study is built on the right foundation from the start.
What scientific questions are these ex vivo models best suited to answer?
TumorGraft3D is best suited to answer questions such as target dependence, free-payload sensitivity, genotype-linked response, cohort-level response patterns, and head-to-head comparison of assets or regimens in the same tumor context.
What endpoints are available in ex vivo studies?
Available endpoints depend on the scientific question. Standard and add-on options can include CellTiter-Glo for comparative sensitivity and rank-ordering, FlowHT for cell populations and immune phenotype, brightfield imaging for morphology, NGS/qPCR for transcriptional response, Luminex/ELISA for cytokines and soluble biomarkers, and Western blot for protein and phospho-signaling readouts.